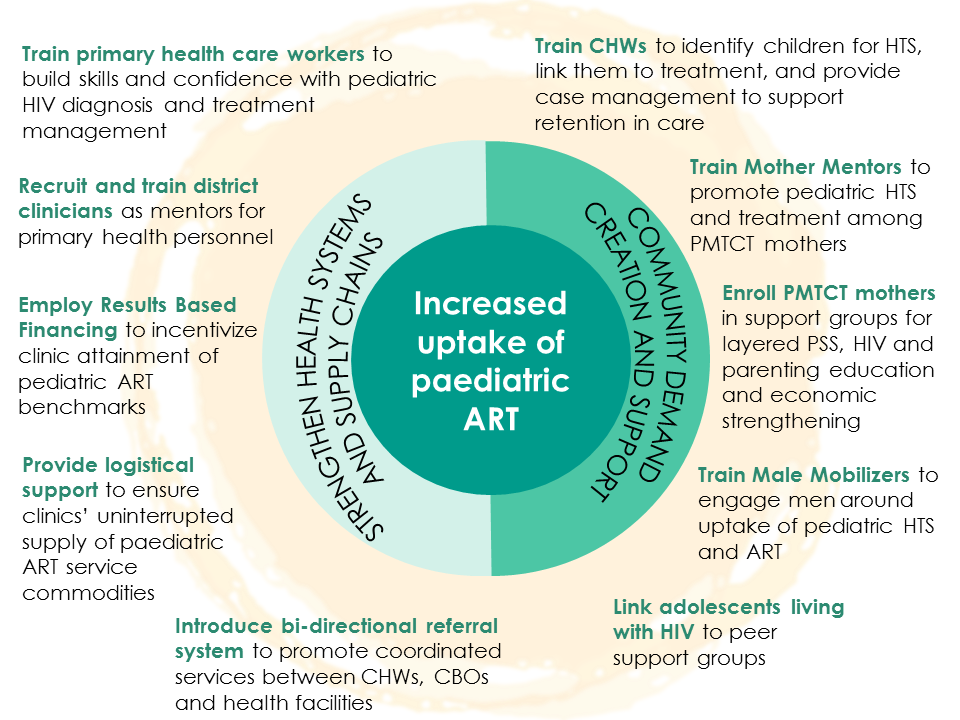
Expanded Integrated Management of Pediatric HIV/AIDS Care and Treatment
Our integrated approach to pediatric antiretroviral therapy provision increased the demand for services at the community level and strengthened local health facilities on the supply side.