
Siyakha Plus: Building Economic Opportunities and Improving HIV Outcomes for Young Mothers and their Children in Mozambique
Creating livelihood pathways for young women has generational benefits. It reduces vulnerability to HIV, early marriage and pregnancy, and gender-based violence; improves health and well-being; and increases economic resilience.
In Mozambique, rates of HIV in pregnant women are highest in women ages 15 to 24. Transmission of HIV from mothers to infants is common due to high rates of unknown status, low rates of antiretroviral therapy adherence, and a lack of adolescent-sensitive care. Social factors like stigma; limited experience caring for children; insufficient nutrition; and limited sexual and reproductive health knowledge such as how to talk about HIV status with partners and access care diminish mothers’ and children’s health and wellbeing.
As a result, rates of HIV positivity, morbidity, and mortality in HIV-exposed infants are high. It is crucial that women with HIV who are pregnant achieve viral load suppression before delivery and adhere to treatment after birth.
Supporting young women through job readiness and employment opportunities can help them protect themselves and their families from these risks. Engaging their families and communities, especially male partners, promotes participation and retention in socio-economic programs and reduces incidences of gender-based violence.
The Siyakha Girls Model
The Bantwana Initiative of World Education’s Siyakha Girls model positions young women to overcome health and socioeconomic challenges. Developed, piloted, and evaluated in multiple contexts based on 10 years of testing and refinement, Siyakha is approved by PEPFAR as a comprehensive economic and resilience strengthening model within DREAMS. World Education is adapting and scaling Siyakha in Malawi, Mozambique, Namibia, South Africa, Zambia, and Zimbabwe.
In Mozambique, we’re piloting Siyakha Plus, an adapted version of Siyakha, among mothers 15-24 living with HIV. Siyakha Plus supports these young women to thrive in the local economy and optimize HIV treatment adherence to reduce transmission to their children. We partner with the private sector to ensure tailored vocational training, entrepreneurship, and employment support rooted in local market opportunities. We collaborate with health authorities to create systems for ongoing, appropriate care and support for young mothers living with HIV.
Siyakha Plus uses an economic platform to layer care and treatment services for young women and their babies. The main interventions focus on:
- Viral suppression through case management; treatment literacy; nutrition; home visits; group mental health support; and health education.
- Keeping babies healthy & HIV-free through breastfeeding; testing referrals; treatment and immunization adherence; and early childhood stimulation and mentoring.
- Economic empowerment through savings and loan groups; business and vocational training; market-based internships; mentoring; start-up kits; and peer support.
The Results
The results from this pilot in Mozambique are promising. Ninety-three percent of participants were actively involved throughout. Eighty-eight percent attended weekly meetings with sessions on treatment adherence, mental health, stigma, and testing and vaccinations for infants.
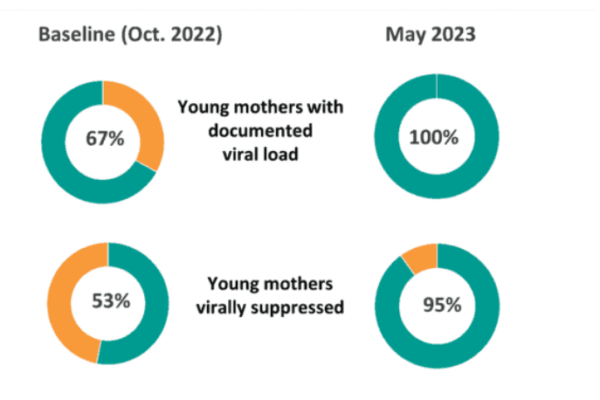
In eight months, 100 percent of the young women had their viral load documented, compared to 67 percent at the start of the pilot; 95 percent achieved viral suppression (from 53 percent); and 100 percent of their children tested negative for HIV on their 18-month confirmatory test.
Peer savings groups accumulated $1400. Eighty-eight percent of participants attended financial literacy courses and 90 percent completed their internships. Participants started a total of 18 group businesses to generate income by the end of the pilot.
The young women improved their skills in childcare, HIV treatment, and business management, and showed increased autonomy and self-esteem.
“I feel healthy physically and mentally by being part of this group. The health of my baby is my top priority, too,” said one.
Health care providers also embraced the pilot:
“… these first four babies that tested negative at this health facility have left a big smile on all the staff and we are now so eager to see the results of the rest of the babies,” said a health director.
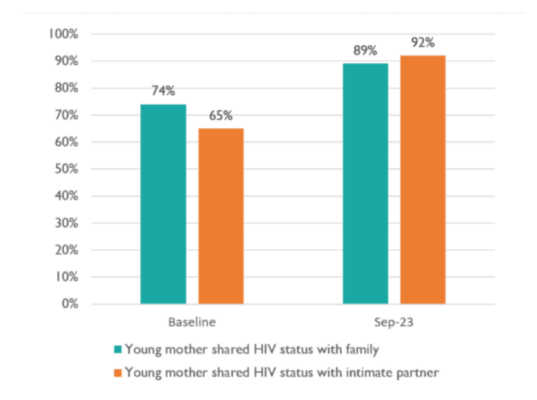
Intimate partner support increased, with more attending health checks, participating in home visits, and starting PrEP to prevent HIV. HIV status disclosure to families and partners increased from 74 to 89 percent and 65 to 92 percent, respectively.
The success of this pilot was due to a number of factors. Cohesive peer groups helped reduce stigma and discrimination and built self-esteem. Economic interventions were effective because of the connection to local market opportunities. The desire to keep infants HIV-free motivated mothers to achieve viral suppression. Personalized support was important, as was an emphasis on multi-sectoral approaches and buy-in from health authorities.
We are using findings from this pilot to refine the Siyakha Plus model, build an evidence base, and disseminate key tools for public use to expand support for young mothers and their HIV-affected children.